
To answer the questions that matter most, we need to identify them and we need to frame them properly. Many of the most critical questions in regards to Lyme disease diagnosis and treatment in our region are not being asked (at least not when, where, or by whom they need to be), are not well framed, are based on poor assumptions, or are all of the above.
In cases where there is information patients don’t have access to, or haven’t found, that would answer these questions, the questions are still essential in seeking it, finding it, or asking for it, as well as for assessing it.
Ticks, it turns out, are a prime example of unasked questions impacting and inhibiting patient care (directly and indirectly, as there are additional paramount influences further discussed in later articles).
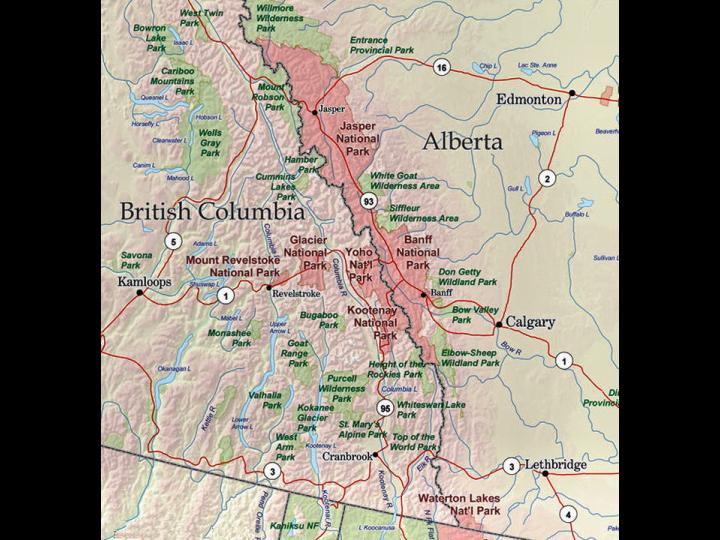
It is, in many states, the perceived lack of deer ticks that is the basis given by doctors as well as state and federal agencies for the lack of Lyme disease (or the lack of even the potential for Lyme disease) in many geographic areas, including the Northern Rockies. This often precludes timely diagnosis and care for patients in these areas (based on policy and guideline factors noted earlier, as well as physician and patient perceptions of the risk of Lyme and their knowledge of symptoms, both of which are lesser in areas not considered to have Lyme disease present).
There many aspects of this issue to discuss, but for now we are using the issue of tick distributions as an example of why the right questions are important (and why a lot more questions should at least be asked). If the presence of deer ticks were a prerequisite for Lyme disease occurrence (it isn’t, but hypothetically), a logical set of questions might include at least the following.
Is a perceived lack of deer ticks a major component or stated component of a state or province’s perceived lack of Lyme disease?
If no:
- Why are states and provinces perceiving it to be via their published resources?
- Why are doctors interpreting this to be a pre-determining factor before considering diagnosis?
If yes:
- Should it be?
- Is this prescribed by current treatment guidelines and/or their interpretation?
- Is this influenced by surveillance guidelines and/or their interpretation?
Do we claim to have reliable knowledge of deer tick and tick species distribution in our region?
If no:

- What are we doing to obtain it?
- How well are we stating our uncertainty and the role it plays in assessing Lyme distribution?
- Are we limiting care based on a factor we cannot properly asses? Is this appropriate? Is this safe?
If yes:
If we think the answer is yes, we need to to think even harder about how and when that information was obtained (having touched even a tiny bit in the preceding post on how expensive and difficult that question would be to discern with reasonable certainty).
- Can we reasonably estimate/predict even the presence/absence of deer ticks?
Assessing with certainty that a species the size of a tick (setting aside for the moment factors such as climate change, human movements, and bird and mammal distributions and movements) is NOT present in a given area would be a monumental task, and would need to be supported by a monumental survey effort.
- Have we attempted to estimate it? If so, how? Is data available? Published?
If a monumental level of survey data is not available, it is probably risky to say the species is not present. In the absence of survey data, it is probably more than risky (see later discussion).
- Is there recent survey data? How (statistically) reliable is it?
If we still state that the species is absent in the absence of surveys or reasonable certainty, we have much bigger questions on our hands, but our questions should also include some of those things we set aside earlier (migrations, climate change, etc.).
Do we actually have reliable Knowledge of deer tick and tick species distribution in our region?
If no:
- Is it reasonable to preclude the presence of Lyme disease, since the absence of deer ticks was the stated rationale?
- How many cases of Lyme could we be missing each year while excluding Lyme from careful consideration based on geography?
- Why is this uncertainty not being implicitly stated?
- Who id leading doctors to believe this certain information? How can that be corrected?
If yes:
- Could the species’ range have changed since our last surveys?
- Could the species range be changing or expected to change in the foreseeable future?
- How will we find the species when it arrives?
But, most importantly, even if we arrived at a hypothetical yes:
- Was our hypothetical assumption that the absence of deer ticks means absence of Lyme accurate?
The answer here is no, discussed below and supported in future articles, as well as peer reviewed articles and studies worth searching for in the mean time, for those interested.
Discussion
No matter what the outcome of these questions, the right questions should include at least the following elements:
- Part of a critical list of questions,
- Built on correct assumptions,
- Properly evaluate the certainty of available information,
- Disclose uncertainties or missing information, and
- Evaluate the risks associated with accepting those uncertainties.
There should be no brief answers to questions as important as these, nor should there be brief statements from agencies and organizations that inherently and improperly imply a degree of certainty that is not justified.
In the case of Lyme disease, there are very few issues that allow for brief answers and statements. This is true for many reasons, but is true based on lack of evidence and lack of information alone. A brief statement about any aspect of Lyme that doesn’t discuss evidence, uncertainty, and remaining questions should, 1) be a serious red flag, 2) not be allowed to be treated as an end to an un-had discussion, 3) not be allowed to replace or negate needed questions, and 4) not be accepted from any entity involved in creation or dissemination of surveillance, diagnosis, or treatment guidelines.
The Deer Tick Example
As a case in point, our example so far assumed that the presence of deer ticks were a necessary prerequisite for the occurrence of Lyme disease (as is the case currently in real life). So additional questions should necessarily include how we know that to be the case and to what degree of certainty. We should see evidence of our health agencies pursuing and providing those answers, which should be leading them to current research that shows it to be untrue and to respond accordingly.
There is too much contrary evidence, it turns out, to warrant maintaining this previous misnomer (also to be discussed in future articles). Multiple species of blacklegged and non-blacklegged ticks have now been demonstrated (and long suspected) to transmit Lyme disease to humans.
As with many aspects of Lyme disease, we often hear or read simple statements made about tick distributions without any qualifying statements, and in my experience so far, without qualifying data, descriptions of, or reference to survey effort. If you were thinking, even remotely, that we’ve done the same here, you are not wrong. This was a discussion of logic and the perils of allowing questions to be wrongly framed and wrongly dismissed. But it did rely on an example that needs a lot more evidence in either direction.
Science doesn’t start with an answer. And we lack the evidence in our region to prove the absence of black legged ticks. And absence of proof is not proof of absence (particularly if no one is looking or not looking adequately). There is evidence that black legged ticks are not mapped in many areas based on lack of survey effort. The nearest example to where I sit being North Dakota, which believed there was not Lyme or black-legged ticks, until they looked this year and found both. There is not evidence that black legged ticks are the only vectors of Lyme disease in humans (there are statements in the past forty years or so indicating or speculating this), but there is copious evidence of the opposite (discussed further in future articles).
Implied Certainty and Unanswered Questions
The issue here is not just that currently published public health information about tick distributions and their relationship to Lyme disease distribution is incorrect. It is also that even if it were correct, it would not suffice to make simple statements with so much at stake and it would not mark the end of the discussion.
The same sadly goes for many statements and many aspects of Lyme disease, which only increases our need to raise awareness and to understand the importance of identifying the right questions (and ensuring they are being asked).
Please stay tuned for future articles and look at our growing site for ways to help us get started, with our first request here and our map location form here.

One thought on “Tick Distributions Example ~ Asking the Right Questions”